

Abstract

Introduction. Transfusion-dependent β-thalassemia (TDT) is the most severe clinical form of β-thalassemia and requires regular long-term red cell transfusions for survival. This study aimed to examine the association of age with the presence of iron overload assessed by Magnetic Resonance Imaging (MRI) and cardiovascular and endocrine complications in TDT patients.
Methods. We considered all TDT patients enrolled in the Myocardial Iron Overload in Thalassemia (MIOT) project at the first MRI examination. Iron concentrations were measured by T2* multiecho technique. All complications were classified according to international guidelines.
Results. Three groups of patients were identified: age<12 years (group 0, N=53), age between 12-17 years (group 1, N=100) and age≥18 years (group 2, N=1857).
The number of transfusional units in the 12 months before the MRI scan resulted significantly lower in group 0 versus both group 1 (20.8±5.3 vs 34.8±10.6; P<0.0001) and group 2 (20.8±5.3 vs 39.2±10.9; P>0.0001) and in group 1 versus group 2 (P=0.021).
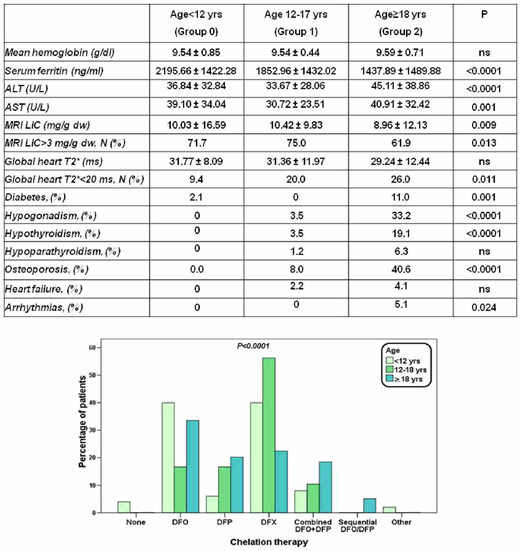
The Table shows the comparison of clinical characteristics among the 3 groups.
Serum ferritin levels were significantly higher in both groups 0 and 1 when compared to group 2. Liver aminotransferases were significantly lower in group 1 than in group 2.
The number of patients with MRI LIC (liver iron concentration) >3 mg/g dw was significantly higher in group 1 than in group 2 and the number of patients with global heart T2*<20 ms was significantly lower in group 0 than in group 2.
Among the endocrinopathies, hypogonadism, hypothyroidism and osteoporosis were significantly less frequent in groups 0 and 1 than in group 2 while diabetes was significantly less frequent only in group 1 when compared to group 2.
Frequency of heart failure was comparable among the groups while the frequency of arrhythmias was significantly lower in group 1 than in group 2.
The types of chelation regimens were significantly different among groups (<0.0001) (see Figure).
Conclusions. Younger patients had more hepatic iron, despite the significant lower transfusional burden. Cardiac iron overload occurs early in TDT patients but it is more frequent in older patients. Endocrinopathies (excluding diabetes) and cardiac complications become clinically evident during the second decade and are time-dependent processes. Our data suggest the need for an effective strategy to prevent iron overload since early childhood, in order to reduce its toxic effect and prevent the development of long-term complications.
Pepe:Chiesi Farmaceutici S.p.A., ApoPharma Inc., and Bayer: Other: No profit support.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal